Posture, etiology of a syndromePaolo
Platania
|
Posturology
guidelines and
interdisciplinary case study |
||||||
|
|
|
|
Posturology
|
The case study
|
The backstage
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Mechanics
The analysis of the Evidences provides consistence to the hypothesis that two simultaneous pathological postural strategies take place in the patient's physiology, the overlapping of which generates all the documented findings. The two postural strategies are well described by the classes:- Head forwarding postural strategy (HFPS): findings sensitive to regression events;
- Mandible retruding postural strategy (MRPS): findings sensitive to orthodontic treatment.
- physically, it is impossible to completely separate the action of either postural strategies on each anatomical district, resulting in partial physical independence,
- logically, their reciprocal independence in onset and subsiding of symptoms and the different goal pursued allows a complete logical independence.
- Findings grouping: grouping the evidences according to their sensitivity to regression events and orthodontic treatment;
- Strategy identification: within each findings group, analysis of the relationship to work out the global strategy and its pathologic goal.
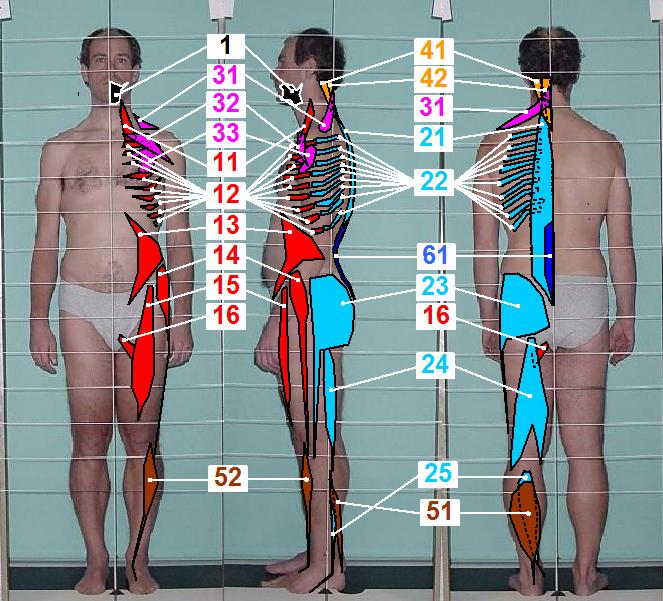
| MECHANICS: Head Forwarding Postural Strategy (HFPS) | ||
| # | Description | |
| Mhfps01 |
Head forwarding postural strategy (HFPS)
Mechanics-evidences relationship: the following list relates the map with the evidences
HFPS is present in the upright as well as in the prone and supine positions, its goal is supposed to be critical since its hyperactive actuator muscles fully inhibit antagonist contraction resulting in pathologic static muscle tone and disabling motor control; nevertheless its pathological action is way far from a randomly unbalanced muscles problem, it rather appears to be a well coordinated reflex, below are described strategy goal and mechanics:
| |
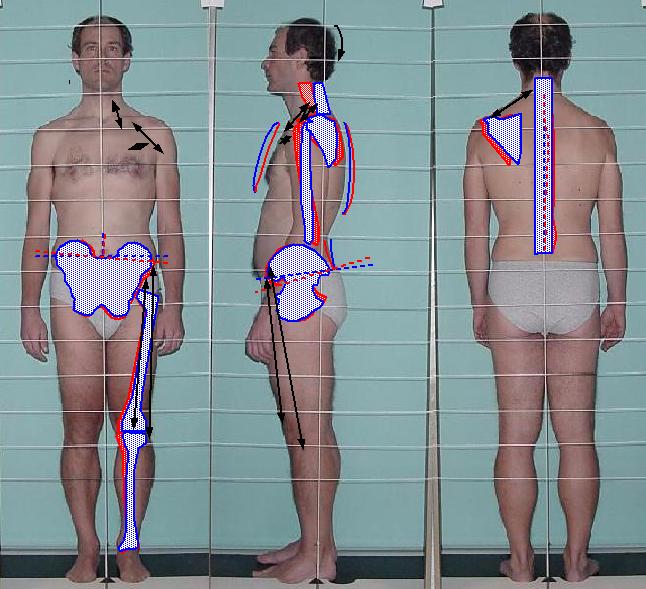
| Mhfps02 | Joint displacement model
Joints physiologic position in the erect station is harmfully affected by HFPS asymmetric torques, its result may be described as:
| |
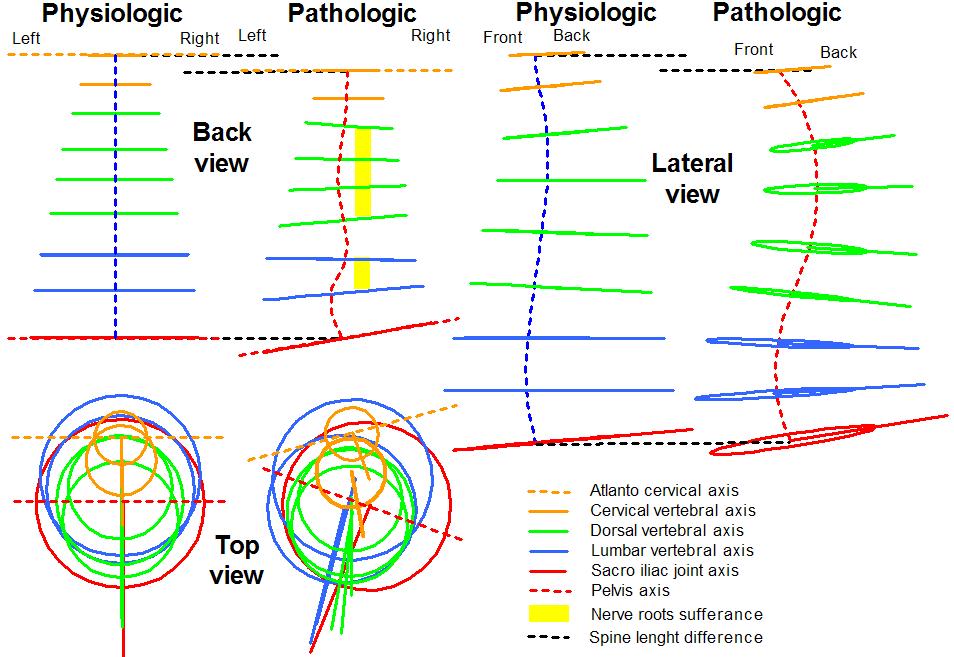
| Mhfps03 | Spine torsional model
HFPS produces strong asymmetric and harmful torque on the spine inducing torsions, scoliosis, and exacerbated curves. The model describes the spine adaptation to HFPS. Pathologic evidences:
|
|
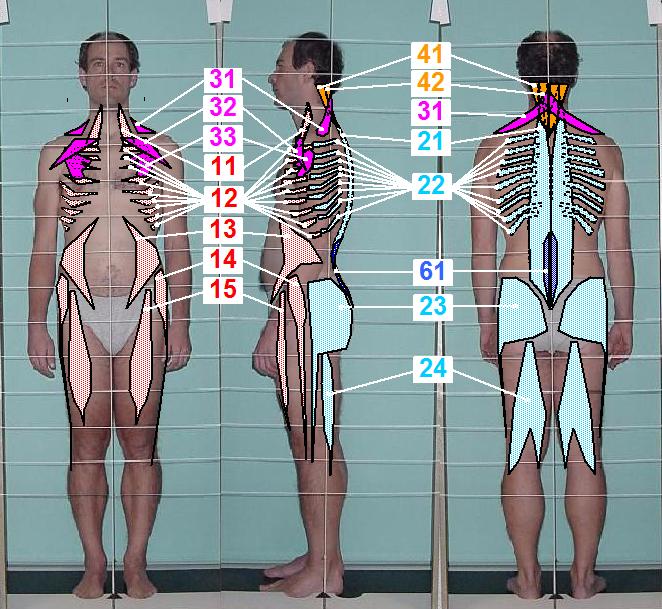
| MECHANICS: Mandible Retruding Postural Strategy (MRPS) | ||
| # | Description | |
| Mmrps01 |
Mandibular retruding postural strategy (MRPS)
Given chronicity and symmetry features, mandible retruding postural strategy (MRPS) is a deviation that is difficult to be aware of, hence, is considered ordinary condition, moreover, the absence of regression events for this type of symptoms and the slowness of improvement during orthodontic treatment don't allow self evaluation to provide significant findings. Fortunately a lot of pre-post orthodontic treatment clues support the described mechanics, furthermore, an acceptable extent of agreement exists in clinic literature to confirm the mechanical hypothesis. All the evidences of MRPS refer to the upright position, nevertheless, its presence in other context (eg. prone and supine) is suspected but this eventuality requires further resources to be investigated; the extent to which MRPS hyperactive actuator muscles inhibit antagonist contraction is lighter than HFPS, the overall result is pathologic static muscle tone but preserved motor control. MRPS is aimed at mandible retrusion (mandible backward motion) for avoiding teeth conflicts, bilateral craniocervical extension (CCE) involvement is supposed to take place for limiting the effect of mandible retrusion (and consequent tongue backward motion) on airflow. Although some features of MRPS appear to be evident, the confidence of the author on all MRPS feature is not as solid as HFPS, hence, each feature is described together with its reliability extent, in other words, some features are evident, some other are uncertain. Evident features:
|
|
|
Bugs report and technical issues notification to the webmaster are highly apreciated
|
| Posture, etiology of a syndrome - ©2008 Paolo Platania |